Atrial Fibrillation – Afib p waves:
Atrial Fibrillation – Important ECG Changes
- Absence of P waves: Instead of discrete P waves, you’ll see irregular, chaotic fibrillation waves.
- Irregular R-R intervals: The distance between consecutive R waves varies irregularly due to the irregular atrial activity.
- Narrow QRS complexes: Generally, the QRS complexes are normal unless there is an underlying conduction abnormality.
- Rapid ventricular rate: Due to the irregular and rapid atrial activity, the ventricular rate is often elevated.
- Absence of PR interval: The irregular atrial activity makes it difficult to discern a consistent PR interval.
These changes reflect the chaotic electrical activity in the atria characteristic of atrial fibrillation.
Overview:
Atrial fibrillation (AF) or Afib stands as the most common sustained cardiac arrhythmia, characterized by irregular and rapid electrical activity in the atria.
Clinical Presentation of Atrial Fibrillation (Afib) :
- Palpitations: Sensation of irregular, rapid, or forceful heartbeat.
- Shortness of Breath: Dyspnea, particularly on exertion, due to compromised cardiac output.
- Fatigue: Persistent tiredness and decreased exercise tolerance.
- Chest Discomfort: Including chest pain or discomfort, often accompanying palpitations.
- Dizziness or Syncope: Resulting from decreased cerebral perfusion during arrhythmic episodes.
When to Suspect Atrial Fibrillation (Afib)?
- Suspect AF in individuals presenting with palpitations, unexplained dyspnea, fatigue, or syncope, especially in those with cardiovascular risk factors or comorbidities.
- Clinical suspicion should prompt further evaluation, including electrocardiography (ECG) and cardiac assessment.
Classification of AF:
1. Paroxysmal Atrial Fibrillation:
- Definition: Atrial fibrillation that terminates spontaneously within 7 days of onset.
- Duration: Typically lasts for seconds to days but usually less than 24 hours.
- Frequency: Episodes may occur intermittently with periods of normal sinus rhythm in between.
2. Persistent Atrial Fibrillation:
- Definition: Atrial fibrillation that sustains beyond 7 days.
- Duration: Requires cardioversion to restore sinus rhythm, either pharmacologically or electrically.
- Recurrence: May revert to sinus rhythm spontaneously but persists longer than paroxysmal AF.
3. Long-standing Persistent Atrial Fibrillation:
- Definition: Atrial fibrillation that sustains for longer than 12 months.
- Treatment challenge: More difficult to achieve and maintain sinus rhythm, often requiring more aggressive therapy.
4. Permanent Atrial Fibrillation:
- Definition: Atrial fibrillation where rhythm control measures have been abandoned, and the patient remains in AF indefinitely.
- Decision: Made when attempts to restore sinus rhythm are deemed impractical or when the patient and physician decide to focus on rate control and symptom management.
5. Nonvalvular Atrial Fibrillation:
- Definition: Atrial fibrillation without significant valvular heart disease (e.g., mitral stenosis, mechanical heart valve).
- Prevalence: Most common form of atrial fibrillation, often seen in patients with hypertension, coronary artery disease, or other cardiovascular risk factors.
6. Valvular Atrial Fibrillation:
- Definition: Afib associated with significant valvular heart disease, such as rheumatic mitral valve disease or mechanical heart valves.
- Management: Requires special consideration for anticoagulation therapy due to increased risk of thromboembolic events.
Diagnosis of AF (Afib):
- Electrocardiography (ECG): Gold standard for AF diagnosis, revealing irregularly irregular R-R intervals and absence of P waves.
- Ambulatory Monitoring: Holter monitoring or event recorders aid in capturing intermittent arrhythmias, especially in cases of paroxysmal AF.
ECG Changes in Atrial Fibrillation (Afib)
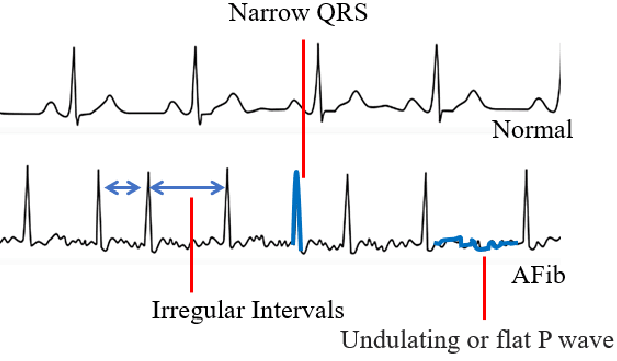
- Absence of distinct P waves.
- Irregularly irregular R-R intervals.
- Narrow QRS complexes in the absence of conduction abnormalities.
Causes of AF (Afib):
- Age: Increasing age is a significant risk factor for AF development.
- Hypertension: Elevated blood pressure predisposes individuals to atrial remodeling and electrical abnormalities.
- Structural Heart Disease: Including ischemic heart disease, valvular heart disease, and cardiomyopathies.
- Hyperthyroidism: Thyroid dysfunction increases sympathetic tone, promoting arrhythmogenesis.
- Obesity: Adiposity is linked to atrial enlargement and electrical remodeling, predisposing to AF.
Signs and Symptoms of Afib:
- Palpitations.
- Dyspnea.
- Fatigue.
- Chest discomfort.
- Dizziness or syncope.
Treatment of AF (Afib):
- Rate Control: Beta-blockers (e.g., metoprolol 25-100 mg twice daily) or non-dihydropyridine calcium channel blockers (e.g., diltiazem 120-360 mg daily) to achieve resting heart rates <80 bpm.
- Rhythm Control: Antiarrhythmic drugs like amiodarone (loading dose 600-1200 mg daily for 1 week, then maintenance dose 200-400 mg daily) or flecainide (loading dose 200-300 mg, then maintenance dose 100-200 mg every 12 hours).
- Anticoagulation: Oral anticoagulants such as warfarin or direct oral anticoagulants (DOACs) like apixaban (5 mg twice daily) or dabigatran (150 mg twice daily) to reduce stroke risk.
Stroke Prevention In AF (Afib):
Let’s See:
stroke prevention in Afib (AF) is crucial due to the increased risk of thromboembolic events, particularly ischemic strokes. The mainstay of stroke prevention in AF involves anticoagulation therapy.
1. Anticoagulation Therapy:
- Oral Anticoagulants: These are the cornerstone of stroke prevention in AF.
- Vitamin K Antagonists (VKAs): Examples include warfarin. Regular monitoring of international normalized ratio (INR) is necessary.
- Direct Oral Anticoagulants (DOACs): Examples include dabigatran, rivaroxaban, apixaban, and edoxaban. They offer fixed dosing without routine monitoring.
- Selection of Anticoagulant: Guided by factors such as stroke risk, bleeding risk, renal function, patient preference, and comorbidities.
2. CHA2DS2-VASc Score:
- Helps stratify stroke risk in patients with AF based on various clinical factors:
- Congestive heart failure
- Hypertension
- Age ≥75 years
- Diabetes mellitus
- Stroke/transient ischemic attack (TIA)
- Vascular disease
- Age 65-74 years
- Sex category (female gender)
3. Bleeding Risk Assessment:
- Tools such as the HAS-BLED score help assess bleeding risk:
- Hypertension
- Abnormal renal/liver function
- Stroke history
- Bleeding history or predisposition
- Labile INR
- Elderly (>65 years)
- Drugs/alcohol concomitantly
4. Risk-Benefit Assessment:
- Balancing stroke prevention with bleeding risk is crucial when deciding on anticoagulation therapy.
- Shared decision-making involving patients in treatment discussions is essential.
5. Non-Vitamin K Antagonist Oral Anticoagulants (NOACs) versus Warfarin:
- NOACs have demonstrated similar or superior efficacy with a lower risk of intracranial hemorrhage compared to warfarin.
- Factors such as renal function, drug interactions, and patient preference influence choice.
6. Considerations in Special Populations:
- Renal impairment: Dosing adjustments may be necessary for certain anticoagulants.
- Elderly patients: Increased bleeding risk and potential benefit from NOACs over warfarin.
- Patients with a history of bleeding: Individualized risk assessment and consideration of alternative therapies.
7. Patient Education and Monitoring:
- Educate patients about the importance of adherence to therapy, signs of bleeding, and regular follow-up.
- Routine monitoring of renal function, liver function, and bleeding parameters may be necessary.
8. Other Measures:
- Control of modifiable risk factors for stroke, such as hypertension and diabetes.
- Left atrial appendage occlusion: Considered in certain patients who are unable to tolerate anticoagulation.
Summary:
Atrial fibrillation poses significant diagnostic and therapeutic challenges, necessitating a comprehensive approach to management. Early recognition, diagnosis, and tailored treatment strategies are paramount in improving outcomes and reducing complications associated with this prevalent cardiac arrhythmia.


Pingback: Atrial Flutter: ECG changes, causes, Treatment - Modern Health
Pingback: Metal Induced Toxicity from Hip Replacement Surgery - Modern Health
Pingback: Common health conditions - MedWebMD