History
A 55-year-old male from the Caribbean presents to the clinic with complaints of fatigue, significant weight loss, and skin lesions that have progressively worsened over the past few months. He also reports intermittent fever and night sweats. The patient mentions a family history of a similar illness in his father, which was never formally diagnosed.
Examination
- General Appearance: The patient appears cachectic and exhibits generalized lymphadenopathy.
- Vital Signs: Blood pressure 110/70 mmHg, pulse 92 bpm, temperature 38.2°C, respiratory rate 18 breaths per minute.
- Skin: Examination reveals multiple hyperpigmented and erythematous plaques distributed across the torso and extremities.
- Cardiovascular: Heart sounds are normal with no murmurs.
- Respiratory: Breath sounds are clear bilaterally, with no wheezing or crackles.
- Abdomen: Palpable hepatosplenomegaly without signs of ascites.
- Neurological: The patient has no focal neurological deficits.
Laboratory Investigations
- Complete Blood Count (CBC): The CBC shows an elevated white blood cell count of 35,000/μL with a significant presence of atypical lymphocytes (blasts). Hemoglobin is 10 g/dL, and platelets are 150,000/μL.
- Biochemical Tests: Laboratory results indicate elevated lactate dehydrogenase (LDH) at 900 U/L and hypercalcemia with serum calcium at 12.5 mg/dL.
- Serology: The patient tests positive for HTLV-1 antibodies.
- Flow Cytometry: Analysis identifies an abnormal T-cell population expressing CD3, CD4, and CD25 markers.
- Bone Marrow Biopsy: The biopsy shows infiltration by atypical lymphocytes.
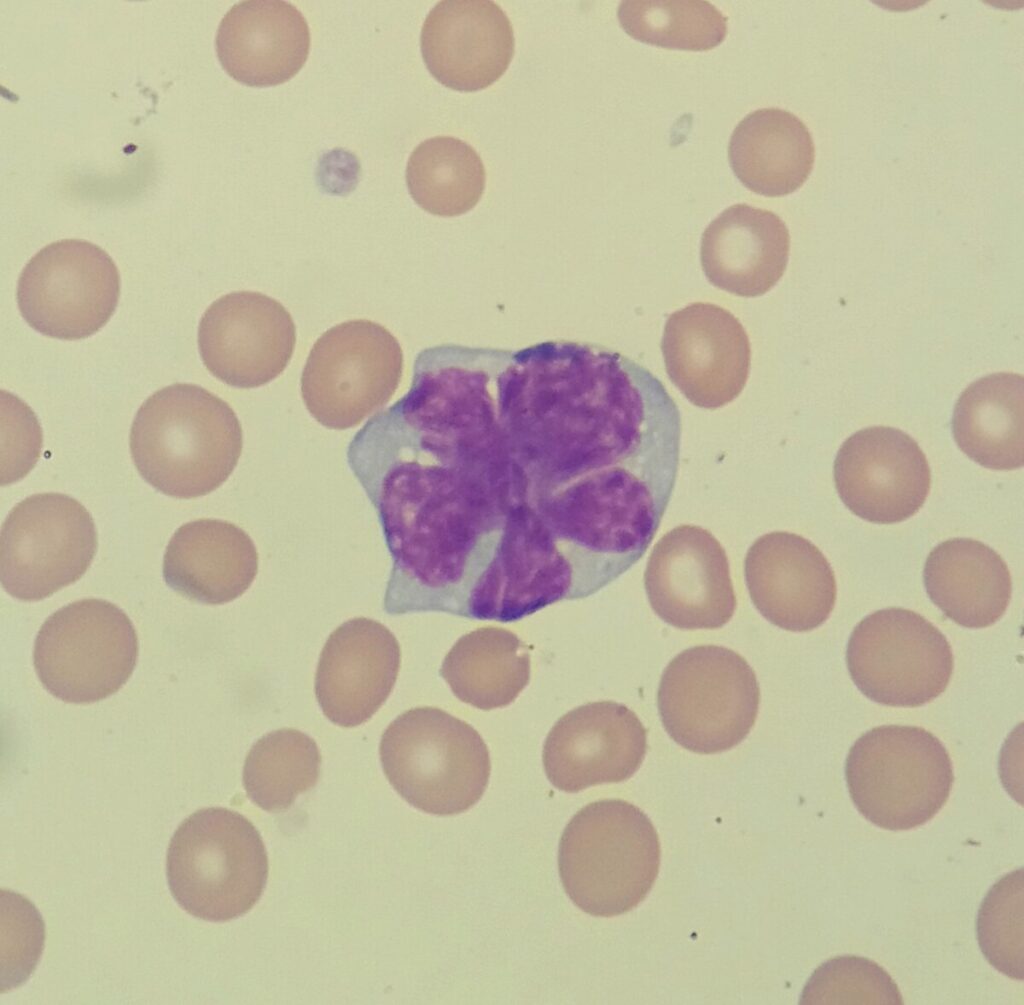
- Peripheral Smear: The peripheral blood smear demonstrates the presence of “flower cells” or “cloverleaf” nuclei, which are characteristic of ATLL.
- Imaging: A CT scan of the chest, abdomen, and pelvis reveals enlarged lymph nodes and hepatosplenomegaly.
Diagnosis
Based on the patient’s clinical presentation, laboratory findings, and serology, a diagnosis of acute ATLL is confirmed.
Overview:
Adult T-cell leukemia/lymphoma (ATLL) is a rare and aggressive malignancy of T lymphocytes associated with the human T-cell lymphotropic virus type 1 (HTLV-1). It is primarily seen in regions endemic to HTLV-1, including parts of Japan, the Caribbean, and Central Africa.
Epidemiology
- Prevalence: Most common in Japan, Caribbean, Central and South America, and parts of Africa.
- Risk Factors: HTLV-1 infection, familial aggregation, and long latency period (often decades).
Pathophysiology
- Virus Involvement: HTLV-1 infects CD4+ T cells, leading to their transformation and uncontrolled proliferation.
- Genetic and Epigenetic Changes: Mutations in genes like TP53, CDKN2A, and epigenetic alterations contribute to malignancy.
Classification
- Clinical Subtypes: ATLL is classified into four subtypes based on clinical features:
- Acute
- Lymphoma
- Chronic
- Smoldering
Management and Treatment
Initial Treatment
- Chemotherapy: Combination regimens such as CHOP (cyclophosphamide, doxorubicin, vincristine, prednisone) are often used.
- Antiviral Therapy: Zidovudine and interferon-alpha may be used to target HTLV-1.
- Supportive Care: Management of hypercalcemia, infections, and other complications.
Advanced Treatment
- Stem Cell Transplantation: Allogeneic hematopoietic stem cell transplantation may be considered in eligible patients.
- Targeted Therapy: Clinical trials investigating novel agents like monoclonal antibodies and small molecule inhibitors.
Prognosis
- Prognostic Factors: Subtype of ATLL, stage at diagnosis, patient’s overall health, and response to initial treatment.
- Survival Rates: Vary widely; acute and lymphoma subtypes have poorer prognoses compared to chronic and smoldering forms.
Follow-Up and Monitoring
- Regular Monitoring: Regular follow-up with clinical evaluations, blood tests, and imaging as needed.
- Management of Recurrences: Repeat biopsies and adjustment of treatment regimens in cases of relapse.
Conclusion
Adult T-cell leukemia/lymphoma is a challenging hematological malignancy with a complex interplay of viral and genetic factors. Early diagnosis and tailored treatment strategies are essential to improve outcomes. Ongoing research into novel therapies holds promise for better management of this aggressive disease.