
Abstract:
Phenytoin, a widely used antiepileptic drug, has a narrow therapeutic index and potential for toxicity when taken in excess. This case study presents a patient with a history of seizure disorder who allegedly consumed multiple tablets of phenytoin. Despite an initially normal examination, neurological signs indicative of toxicity developed by the second day of observation. This highlights the delayed presentation and importance of continued monitoring in phenytoin overdose.
Patient Profile:
- Age/Gender: 28-year-old male
- Past Medical History: Known case of seizure disorder
- Medication History: On regular phenytoin therapy (dosage unknown)
- Presenting Complaint: Alleged ingestion of multiple phenytoin tablets
- Time of Presentation: Within 6 hours of ingestion
Day 1 – Initial Assessment:
- Vital Signs:
- Blood Pressure: 120/80 mmHg
- Heart Rate: 82 bpm
- Respiratory Rate: 16/min
- SpO₂: 98% on room air
- Temperature: Afebrile
- General Physical Examination:
- Patient was conscious, alert, and oriented to time, place, and person
- No signs of respiratory compromise or circulatory instability
- No external injuries or signs of trauma
- Central Nervous System (CNS) Examination:
- GCS: 15/15
- Cranial Nerves: Intact, pupils equal and reactive to light, no diplopia, normal extraocular movements
- Motor System: Normal bulk, tone, and power in all four limbs (5/5)
- Reflexes: Physiological, plantar flexor bilaterally
- Sensory System: Intact to light touch, pain, and temperature
- Cerebellar Signs: Not present
- No signs of meningeal irritation
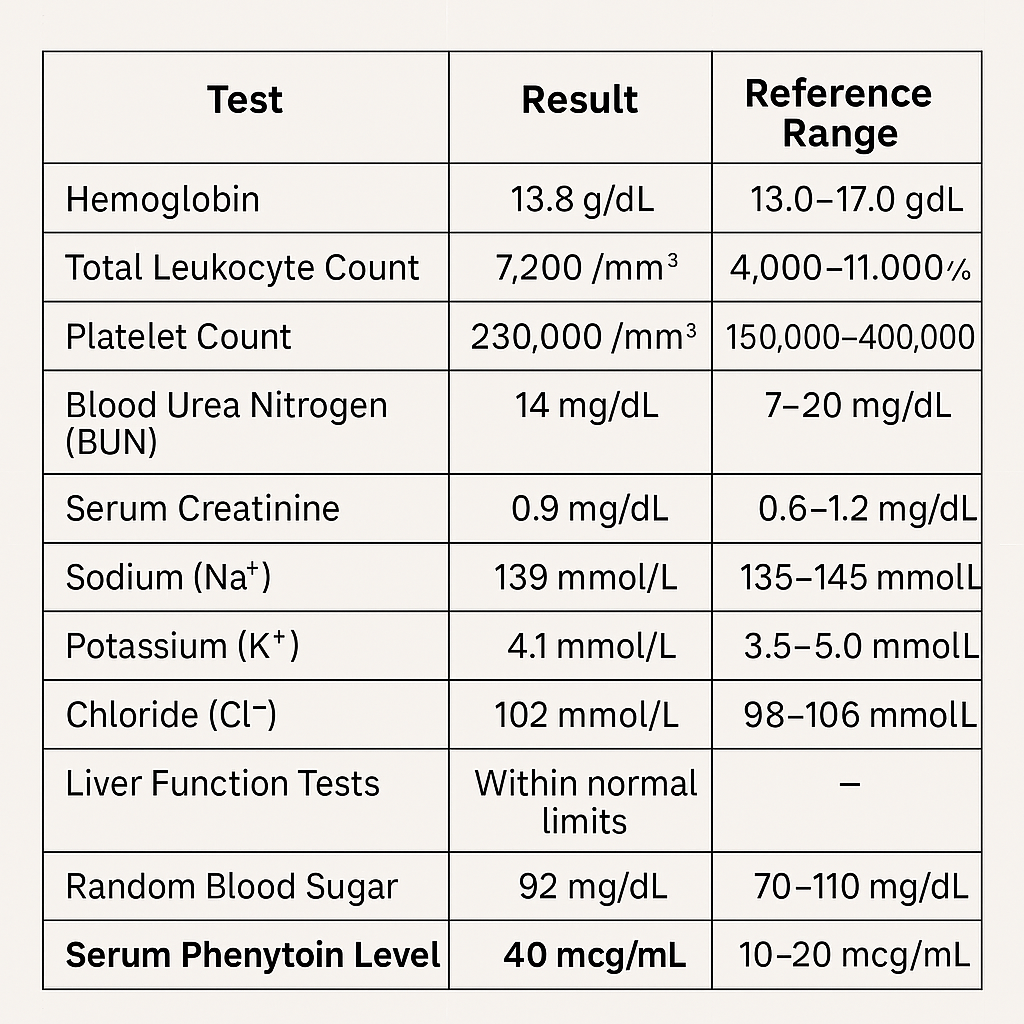
- Laboratory Investigations:
Day 2 – Clinical Progression:
- CNS Examination (Detailed):
- Consciousness: Drowsy but arousable to verbal and tactile stimuli
- Behavior: Hyperactive movements noted on stimulation, otherwise subdued
- Cranial Nerves:
- Horizontal gaze-evoked nystagmus bilaterally
- Pupils equal and reactive
- No facial asymmetry
- Normal gag reflex
- Motor System:
- Normal tone and bulk
- Mild tremors on movement
- Power preserved (5/5) in all limbs
- Reflexes: Brisk deep tendon reflexes, plantar response flexor
- Cerebellar Examination:
- Ataxia on attempting to stand and walk; required support
- Dysmetria on finger-to-nose testing (past-pointing present)
- Positive heel-to-shin incoordination
- Intention tremor noted on reaching movements
- Dysdiadochokinesia present
- Sensory System: No deficits detected
- Speech: Mild scanning dysarthria
Interpretation:
The patient’s neurological deterioration on Day 2 correlates with the supratherapeutic phenytoin level. Symptoms such as nystagmus, ataxia, intention tremor, and drowsiness are classical features of phenytoin toxicity, particularly cerebellar involvement.
Management and Outcome:
- Patient was managed conservatively with supportive care
- Phenytoin was withheld, and levels were monitored
- Adequate hydration and monitoring of vital and neurological signs were continued
- Gradual clinical improvement noted over the following days
Conclusion:
This case exemplifies the potential for delayed onset of toxicity following phenytoin overdose. Even with initially normal findings, high serum levels may manifest neurological symptoms after redistribution. Continuous monitoring and early detection are key to managing such cases effectively.